Chondromalacia Supplementation Considerations
Regarding Chondromalacia Patellae, I will briefly address the state of supplementation science, my clinical experience with supplementation for joint pain, and then go over the bigger picture of body inflammatory state, hydration, and neuro structural considerations. This information is not a substitute for seeing your health care practitioner; and is my opinion.
Joint Supplement Science
There are actually a handful of controlled double-blinded studies on glucosamine, chondroitin, MSM and Boswellia. Here is a recent one:
Adv Ther. 2011 Oct;28(10):894-906. Epub 2011 Oct 7
The problem is that the vast majority are for Osteo Arthritis, which is a very advanced and difficult to treat form of joint damage. They also never exclude NSAID use, and NSAIDS inhibit cartilage repair. With any sort of inflammatory disorder the supplement with the greatest quantity and quality of science behind it by far is fish oil. EVERYONE should supplement with fish oil.
Joint Supplement Clinical Observations
I have about thirty years clinical experience with the various supplementation schemes for joint issues. Here are my observations:
Chondroitin and Glucosamines - These sulfur-bearing biological polymer building blocks rarely give good results; and I have seen allergic reactions too often. This likely due to high sulfite content and the fact that most are derived from shellfish. I never recommend these anymore.
Boswellia works well for some people, but is definitely hard on the gut. Many people have gut issues taking Boswellia. It is a less strong cyclo-oxygenase inhibitor and seems to have a similar action to NSAIDS, anti-inflammatory but doesn't seem help joint rebuilding directly.
Kaprex - A hops, rosemary and olive leaf extract that works well for some people, but not others. I believe this to be due to variations in the underlying cause - If you have chondromalacia patellae due to an underlying pro-inflammatory state then Kaprex works great. No gut problems with Kaprex, but it is expensive.
Aloe Vera - The allantoin in Aloe has been shown to increase cell turnover. This can be helpful to speed up cartilage repair.
Runner's Edge - An antioxidant enzyme supplement that will clear grit out of joint fluid in the knees if you give it time.
ACUTE - Another effective enzyme supplement, this one focused on breaking down the protein signaling molecules to mitigate the inflammatory cascade. A great alternative to NSAIDS without any liver or kidney toxicity.
Vitamin D - Best from the sun, essential for normal immune function.
Hayaluronic Acid - Pulls moisture into the tissues. Best from food.
MSM - Methy Sulfonyl Methane - basically a highly-bioavailable form of Sulfur. My favorite, about 80% of people who use it notice a positive improvement. Easy to use, just buy it in bulk and mix with water. Inexpensive too, but just don't bother with the chinese-sourced stuff, not worth it. If you aren't low in sulfur, MSM may not help. People who respond to chondroitin/glucosamine typically respond even better to MSM by itself. If you are, it will soften up and hydrate scarred-up and thickened connective tissue and improve cartilage repair rates.
The above is not a complete nutrient list for cartilage repair - other known nutrients for cartilage repair include vitamin C, zinc, copper, and manganese.
Pro Inflammatory State and Knee Pain
Sometimes the knee is just where the inflammation is being expressed. A diet high in Omega-6 fatty acids and refined carbohydrates and/or excessive calories are all associated with a pro-inflammatory balance. Some other factors that promote inflammation in the body include food allergies, impaired detoxification pathways, acidity, and chronic infections.
Hydration
You need both general hydration and local hydration. By local hydration I mean inside the cartilage itself. Two known factors here. One is Hayaluronic
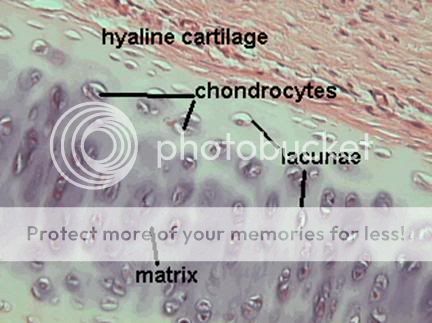
Acid, it pulls moisture into the tissues. Best food source known for hayaluronic acid is any stock made from bones (also available as a supplement). The second factor is the mechanical action of the joint. Joint cartilage, known as Hyaline cartilage is a like a very smooth and slippery sponge. Like all connective tissue it is living cells within a non-living matrix:
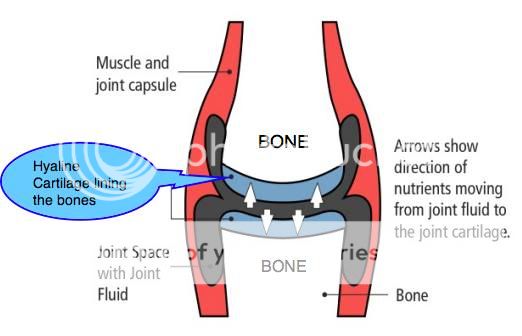
You can see that in this matrix the cells have a little space like a pool that they live in called lacunae. Important fact: Hyaline cartilage contains no blood vessels! The only way those cells get the oxygen, blood sugar, and nutrients they need to survive and thrive is to absorb the joint fluid directly:
This is called imbibition, the direct drinking of water. When you put weight on your knee, it compresses the cartilage "sponge" and squeezes water and waste material out. When you pick up your leg, it de-compresses the "sponge" allowing it to absorb water and nutrients again. This is essential for the normal nightly burst of cartilage repair in the body.
Neuro-Structural Integrity
If you knee is misaligned, it can be compressed in one area and not another. This spot will have accelerated cartilage wear, and reduced repair because it is not decompressing and getting the imbibition it needs. Often knee alignment is secondary to hip and low-back alignment, which is secondary to neck alignment.
If your neck is missing it's natural curve, that puts tensile stretching forces on the spinal cord, which usually increases nerve tension throughout the body. Since nerves cross joints, and the spinal cord is more important tissue than a knee, the body will compress the knee trying to reducing the pulling on the spinal cord. In this case the entire knee may not effectively decompress at all.
It may sound strange how having a good chiropractor work on your spine can improve knee pain, but I hear my clients tell me how much better their knees are time and time again.
Review
So I have discussed the science of joint supplementation, my clinical observations with joint supplementation, as well a discussion of other factors like the overall tendency to inflammation in the body, hydration, as well as effects of loss of neuro-structural integrity.
One last point: The side-by-side RV knee straightening factor is real, and makes a big difference.
Yours in Health,


") .
.